I’m happy to join the rest of the gout world in announcing new gout guidelines for 2012 from our friends in the American College of Rheumatology (ACR).
I’m less than happy about some aspects of the guidelines. But I’ll save my moaning for another day when I’ve had more time to reflect on the entire content of the two-part report. The total report covers 31 dense pages, so it might take a while. On the other hand, the key points are covered in a single page press release from the author’s publishers.
I’m sure you will see this press release, and comments on it on a host of other gout websites, and news websites. Unlike other commentators, I will not simply copy the press release without a little explanation. I certainly won’t be following other commentators and giving you the publisher’s paid links to the full reports. I’ll give you the full gout guidelines for free below.
The Task Of Investigating Gout Guidelines
The task of leading the investigation into new gout guidelines falls to lead investigator John D. Fitzgerald, MD, Ph.D., Acting Rheumatology Division Chief at the University of California, Los Angeles (UCLA). He tells us:
“In order to improve patient care, the ACR funded this collaborative effort among U.S. researchers to produce guidelines, outlining pharmacological therapies and non-drug treatments to manage gout.”
Thus, we end up with a 33-strong committee, sorry, Task Force Panel, who have produced the two-part 2012 Gout Guidelines. Part 1 is about managing high uric acid, and Part 2 is about treating gout pain. The committee gave them longer titles, (so they could each add a word?), but I’ll save you from that for now.
High Uric Acid Guidelines
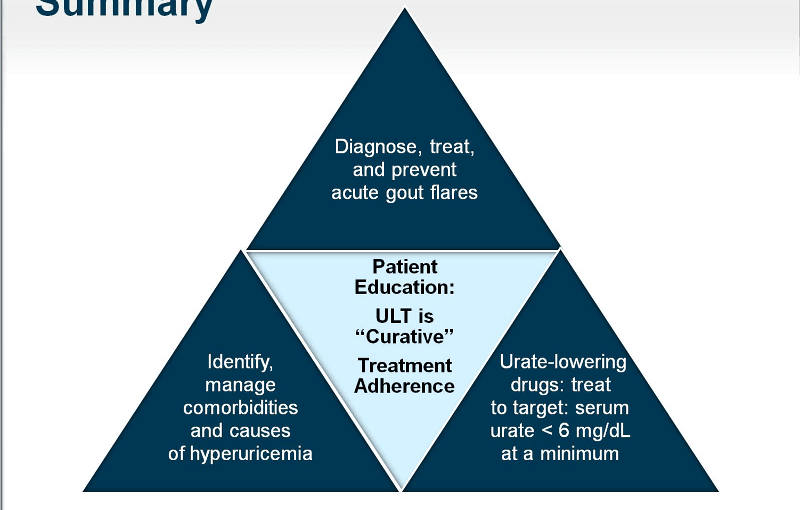
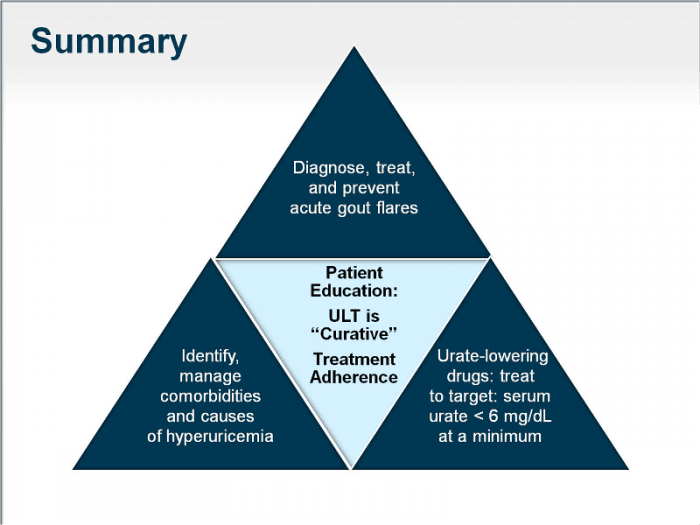
My summary of the press release summary of the first report summary is:
- Educate patients about: diet; lifestyle choices; treatment targets, and management of coexisting diseases
- Recommend specific dietary items to encourage, limit, and avoid.
- Treat patients with uric acid lowering therapy using Xanthine Oxidase Inhibitors (XOIs): allopurinol or febuxostat.
- Lower uric acid levels to less than 6 mg/dL.
- Start allopurinol dose no greater than 100 mg/day, and less for patients with chronic kidney disease. Increase dose to achieve target, which can exceed 300 mg even in those with chronic kidney disease.
- Pre-screen patients at high risk for severe allopurinol side-effects (e.g., Koreans with stage 3 or worse kidney disease, and all those of Han Chinese and Thai descent).
- Prescribe combination therapy, with one XOI and one uriocosuric agent, when target uric acid levels are not achieved. Consider pegloticase in patients with severe gout disease who do not respond to appropriate doses of uric acid lowering treatment.
Not a single mention of liver function and kidney function tests during uric acid treatment. Patient beware!
Treating Gout Pain Guidelines
My summary of the press release summary of the second report summary is:
- Start drug therapy within 24 hours of the start of an acute gout attack.
- Continue uric acid lowering treatment, without interruption, during acute gout flares.
- Use Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), corticosteroids, or oral colchicine as first-line treatment for acute gout. Use combinations of these medications for severe or unresponsive cases.
- If tolerated and safe with any other medicines, use oral colchicine or low-dose NSAIDs to prevent gout attacks when starting uric acid lowering treatment.
Dr. Fitzgerald concludes:
“The ACR gout guidelines are designed to emphasize safety, quality of therapy, and to reflect best practice based upon medical evidence available at this time. Our goal is that these guidelines, along with educating gout patients in effective treatment, will improve adherence, quality of care and management of this painful and potentially chronically debilitating condition.”
That being the case, one wonders why they didn’t take more notice of my Best For Gout articles[1]. I will point out where you can discuss improvements to these guidelines with your doctor when I complete my full review.
Gout Guidelines: Next Steps
These gout guidelines are a great starting point for discussing gout management with your doctor. You should always insist on a personal treatment plan. Once you get that, if you are unsure on any points, you can ask in the gout forum.
If you want to discuss the full gout guidelines, both parts are currently linked from the front page at rheumatology.org. Specifically:
- Khanna, Dinesh, John D. Fitzgerald, Puja P. Khanna, Sangmee Bae, Manjit K. Singh, Tuhina Neogi, Michael H. Pillinger et al. “2012 American College of Rheumatology guidelines for management of gout. Part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia.” Arthritis care & research 64, no. 10 (2012): 1431-1446. (rheumatology.org/practice/clinical/guidelines/Gout_Part_1_ACR-12-0014.pdf)
- Khanna, Dinesh, Puja P. Khanna, John D. Fitzgerald, Manjit K. Singh, Sangmee Bae, Tuhina Neogi, Michael H. Pillinger et al. “2012 American College of Rheumatology guidelines for management of gout. Part 2: therapy and antiinflammatory prophylaxis of acute gouty arthritis.” Arthritis care & research 64, no. 10 (2012): 1447-1461.(rheumatology.org/practice/clinical/guidelines/Gout_Part_2_ACR-12-0013.pdf)
I have reviewed the principles of the official rheumatologist guidelines in ACR Gout Management Principles. I look forward to hearing your views on gout guidelines in Improving Gout Management Principles for Gout Sufferers.
Leave Taking Gout Guidelines To Task to continue your GoutPal Plan for Gout Students.
Taking Gout Guidelines To Task Comments
GoutPal visitor responses and associated research include:
2020 Gout Summary
Since I started this gout summary project based on the 2012 gout guidelines, there have been several professional recommendations. The latest of which is 2020 Gout Management Guideline. So I am reviewing all aspects of the gout summary with updates where necessary.
If you spot any outdated references to 2012 guidelines, please let me know. It’s best to discuss guidelines in the gout forum. But if you won’t use forums, please use the feedback form below.
Gout Guidelines References
- Taylor, Keith. “Best For Gout.” GoutPal.com 2012-2017. Now at Best For Gout Archive. Also search GoutPal for current “Best For Gout” articles.
Please give your feedback
Did this page help you? If yes, please consider a small donation. Your donations help keep GoutPal's gout support services free for everyone.
If not, please tell me how I can improve it to help you more.
- YouTube
- The gout forums.










